Key Takeaways
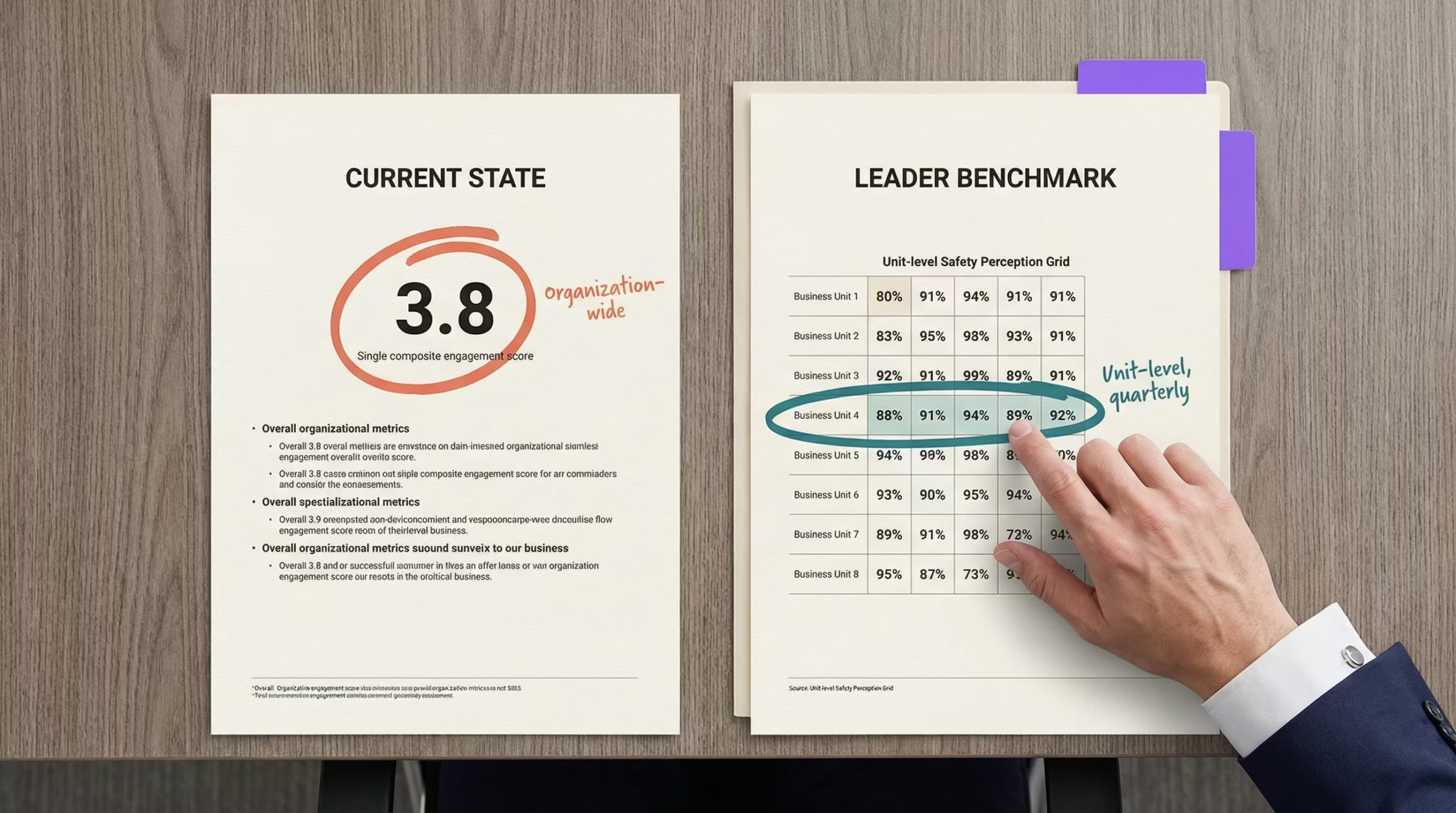
- Leading CHROs measure safety perception at the unit level quarterly, while most programs still rely on annual engagement composites that mask the units in crisis
- The gap between leaders and most programs comes down to whether perception data is connected to intent-to-stay, turning it from a culture metric into a workforce planning tool
- Peer organizations that acted on perception data saw measurable retention improvements within 90 days of establishing baselines
Every CHRO in behavioral health knows safety concerns drive turnover. The difference between the CHROs who keep losing staff and those who’ve stabilized their hardest units isn’t awareness of the problem. It’s what they measure and when they measure it.
This piece shows what peer CHRO safety insights reveal about how leading behavioral health organizations track safety perception differently, and where most programs fall short. For the full research behind why perception predicts retention, see the complete guide to staff safety in psychiatric hospitals.
What Peer CHRO Safety Insights Reveal About Measurement
The operational gap between leading programs and most behavioral health HR operations shows up across four dimensions. In each case, the difference isn’t budget or technology. It’s measurement precision and speed.
Measurement level: unit vs. composite. Most CHROs review safety perception as part of a facility-wide engagement score. Leaders pull safety-specific items and score them by unit. The difference matters because a facility might report 72% positive safety perception overall while one behavioral health unit sits at 41%. That unit is a retention emergency, invisible in the composite. How to build this measurement framework covers the specific instruments and delegation structure.
Measurement frequency: quarterly vs. annual. Most programs measure safety culture once a year through their engagement survey. Leaders run quarterly pulses on safety perception specifically, capturing directional trends that predict retention shifts 90 days out. Annual measurement can only confirm what already happened. Quarterly measurement surfaces what’s about to happen.
Data connection: standalone vs. correlated. Most programs treat safety perception as a standalone culture metric. Leaders connect perception scores to intent-to-stay data at the unit level, which turns safety perception into a workforce planning tool their CFO can act on. The facilities that made this connection recorded intent-to-leave dropping from 22% to 7% [1].
Onboarding attention: ignored vs. tracked. Most programs wait for the annual survey to capture new hires’ safety perception. Leaders measure perception during the first 90 days of onboarding, because a new nurse’s sense of whether the organization takes safety seriously forms fast and is remarkably durable once set. The CHROs ahead of the curve treat that onboarding window as the highest-leverage moment for perception formation.
Where Leaders and Most Programs Compare
| Dimension | Most Programs | Leading Programs |
|---|---|---|
| Measurement level | Facility-wide or organization-wide composite | Unit-level, scored separately from engagement |
| Measurement frequency | Annual (buried in engagement survey) | Quarterly safety-specific pulse + annual full assessment |
| Retention connection | Safety perception and turnover tracked separately | Perception scores correlated with intent-to-stay by unit |
| Onboarding perception | First captured at annual survey | Measured within first 90 days |
| Action on data | Survey results reviewed and filed | Unit-level declines trigger CSO coordination and charge nurse coaching |
| Financial framing | Safety positioned as a wellness benefit | Safety framed as workforce planning investment with per-point ROI |
The financial framing matters for the CFO conversation. Each percentage point of nursing turnover costs roughly $289,000 annually [2]. Leaders don’t present safety perception as a culture initiative. They present it as the leading indicator that explains why their next quarter’s turnover moved, with the full retention data to back it up.
“The CHROs pulling ahead aren’t measuring turnover more carefully. They’re measuring something upstream: the safety perception shift that predicts turnover months before a resignation letter arrives.”
Ready to see where your program stands against peer benchmarks?
Assessing Where Your Program Stands
Run through this self-check against the leader benchmarks above. Be honest about where your program sits today.
- Can you pull unit-level safety perception scores right now, or would you have to dig through a composite engagement survey?
- Do your safety perception scores connect to intent-to-stay data, or are they standalone metrics?
- When was the last time a unit-level perception decline triggered a specific intervention (not a policy review, but a visible action staff could see)?
- Do new hires on behavioral health units get a safety perception check within their first 90 days, or do they wait for the annual survey?
- Can you tell your CFO the annualized cost of turnover on your highest-risk unit in a single number?
If more than two answers point to the “most programs” column, that’s the gap. The HR brief on safety perception metrics provides the specific data points to start closing it.
One finding worth flagging: facilities that run safety culture surveys without visibly acting on results see declining response rates and worsening scores [3]. Measurement without visible follow-through is counterproductive. The programs achieving leader-level results pair measurement with action staff can see. Peer CNOs tracking unit-level data describe the same pattern from the clinical side.
Pull your safety-specific items from your engagement survey and score them by unit. That single step, done this week, tells you whether you’re operating as a leader or running the same measurement approach as everyone else. The CHROs who stabilized their behavioral health units started with that one data pull. Within 90 days, they had the peer CHRO safety insights that changed the retention conversation entirely.
PEER BENCHMARKS
See How Your Safety Perception Program Compares
Leading behavioral health CHROs are using perception measurement as a workforce planning tool. Find out where your program stands.
References
- ROAR for Good. Internal data, 2024. Internal data
- NSI Nursing Solutions. 2025 NSI National Health Care Retention & RN Staffing Report. https://www.nsinursingsolutions.com/documents/library/nsi_national_health_care_retention_report.pdf
- AHRQ PSNet. Culture of Safety. https://psnet.ahrq.gov/primer/culture-safety